Faxing a referral in 2026 is still the norm. The fax goes out. No confirmation comes back. Someone calls. Someone leaves a voicemail. The patient shows up at the specialist's office ten days later, and tells their story from scratch.
That's not a technology problem. It's a workflow problem. And in personal-injury care chains, where a single patient moves across a chiropractor, orthopedist, pain management provider, and spine surgeon inside the same episode of care, it compounds at every handoff.
By the time a patient reaches a spine surgeon, the referring chiropractor's intake findings, the orthopedist's imaging notes, and three weeks of symptom progression may exist somewhere — but not anywhere the surgeon can access before the appointment. The context evaporated somewhere between the fax machine and the front desk.
The Personal-Injury Chain Has a Structural Referral Problem
Patients in personal-injury cases don't choose their care team from a directory. They get referred across providers in a coordinated sequence, each handoff is supposed to carry clinical context forward. In practice, it rarely does.
The reasons are predictable:
- Fax and phone are asynchronous by design. You send; you hope. There's no status update, no confirmation that the referral was received, no alert when the patient actually gets scheduled.
- Each practice runs its own intake process. The patient fills out a new form at every stop. The chiropractor's findings don't automatically land in the orthopedist's intake. The orthopedist's imaging notes don't reach the pain management provider unless someone manually faxes them.
- Referral reason gets lost or abbreviated. What the referring provider actually wanted the specialist to know, the specific mechanism of injury, the symptom pattern, the urgency indicators, often gets reduced to a checkbox or dropped entirely.
The result is referral leakage: patients who fall out of the care chain because an appointment never got scheduled, a specialist who treats the patient as a new case with no prior context, and referring providers who have no visibility into what happened after the handoff.
For practices managing a personal-injury caseload, this isn't an occasional inconvenience. It's the standard operating condition.
What a Doctor-to-Doctor Referral Should Actually Do
A referral isn't a piece of paper — or shouldn't be. It's a clinical handoff. It should carry three things:
1. Why this patient is being referred — the specific reason, not just a diagnosis code
2. What the receiving provider needs to know — relevant history, assessment findings, documents
3. Confirmation that the handoff worked — the patient is connected, the appointment is scheduled, the loop is closed
The fax-and-phone workflow delivers none of these reliably. It delivers a document and a hope. Replacing fax referrals in healthcare with a tracked, context-carrying digital flow isn't a convenience upgrade — it's how a care chain actually functions as a team.
How PatientPreVue Handles the Referral Handoff
PatientPreVue's digital referral system for chiropractors and specialists was built around the actual handoff problem, not just the document transmission problem.
Encrypted Referral Reason
When a provider initiates a referral through PatientPreVue, they include the referral reason in the referral itself — encrypted, specific, and structured. Not a fax cover sheet with "please see patient." The receiving specialist gets the actual clinical context: why the patient is being referred, what the referring provider observed, what they want the specialist to assess.
That context arrives before the patient does.
Automatic Patient-Specialist Connection
When a referral is sent, the patient is automatically connected to the receiving specialist within the PatientPreVue network. There's no separate step where
the patient has to register with a new provider, no gap where the specialist can't access the patient's records because they're not yet connected. The connection happens as part of the referral itself.
That means the specialist can review the patient's organized records library and prior intake assessments before the appointment — not after the patient finishes filling out a new form in the waiting room.
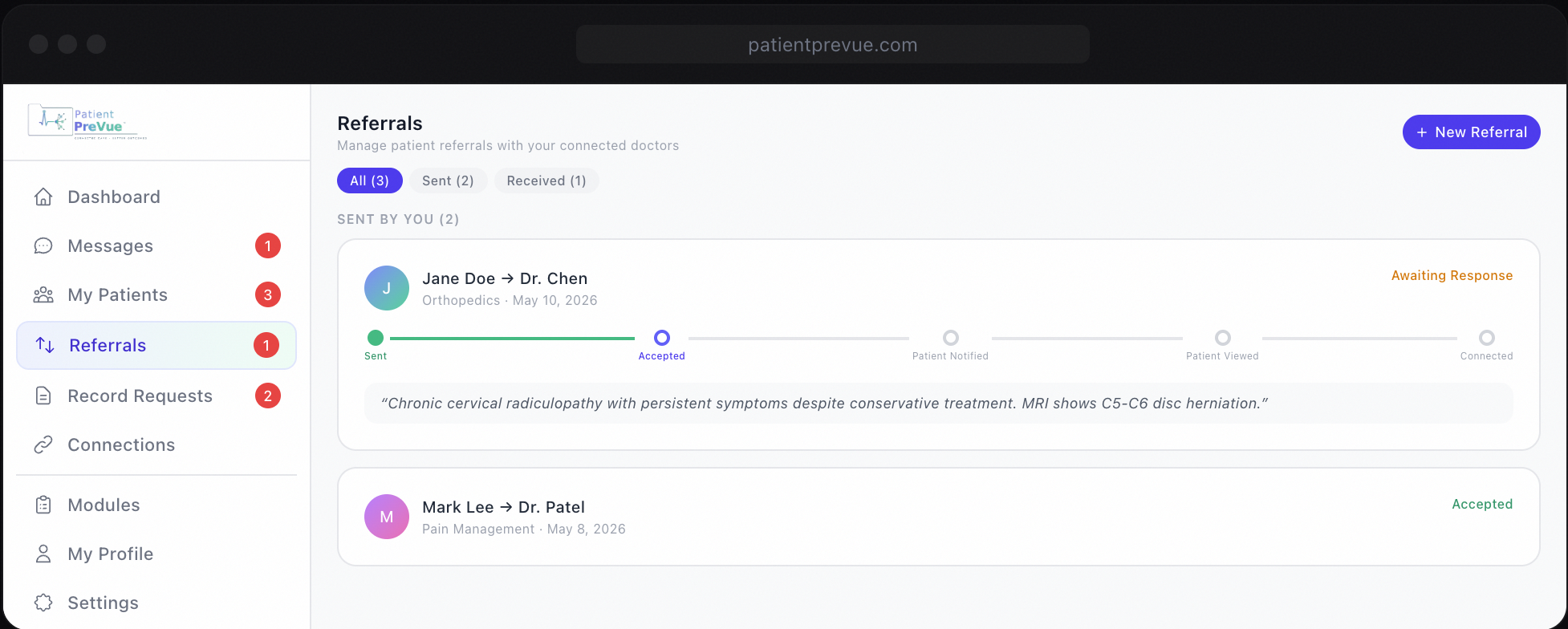
Step-by-Step Referral Progress Tracking
No more chasing a fax confirmation. The referring provider can see exactly where the referral stands: referred, accepted by the specialist, viewed, patient connected. Every party — referring provider, specialist, and patient — has visibility into where things are.
This matters operationally. A chiropractor managing a dozen active personal-injury cases needs to know which referrals have been accepted and which are sitting unanswered. A patient needs to know their specialist appointment is actually happening. Right now, that visibility doesn't exist. The fax went out — that's all anyone knows.
Referral tracking for personal injury practices means closing that gap: a real-time status at every stage of the specialist referral workflow, visible to everyone in the chain.
The Records and Summaries That Travel with the Referral
A referral with context is only as good as the context the specialist can actually access. PatientPreVue's referral flow is designed to work alongside the records library and AI-generated summaries — so the specialist isn't just getting a reason for the referral, they're getting the full picture.
Records Library
Patients upload and organize their records — imaging, prior visit notes, legal documents, insurance correspondence — in a structured library. When a referring provider sends a referral and the patient is connected to the specialist, those records are available for the specialist to access (with the patient's sharing controls in place).
The specialist sees organized, filterable documents — not a fax packet or a stack of PDFs with no labeling. Learn how patients manage and share their records on PatientPreVue.
AI-Generated Summaries
PatientPreVue generates two summary formats from each intake assessment: a tiered clinician overview that surfaces urgent indicators, notable findings, and background information in a structured hierarchy, and a first-person narrative that captures the patient's own account of their symptoms and history.
When a patient completes intake before a specialist appointment, the specialist gets that summary before the visit. The intake is already done. The history is already documented. The provider can spend appointment time on the clinical work — not on reconstructing context the patient already provided somewhere else.
Personal Injury Care Coordination: Be Part of the Team Around Your Patient
Personal-injury cases are team cases. A chiropractor who initiates care, an orthopedist who manages the musculoskeletal findings, a pain management provider handling symptom control, a spine surgeon evaluating for intervention — these providers are functionally a care team, even if they've never coordinated directly.
The problem is they don't have a shared workspace. They operate in separate systems, communicate by fax, and rely on the patient to carry their own history from stop to stop. The patient becomes the medical record — and a fallible one at that.
PatientPreVue gives that care team a shared layer. Not a new EHR that everyone has to adopt. A connected-care layer that sits above the systems they already use — where referrals carry context, records travel with the patient, and every provider in the chain can see what the others have documented (within the patient's sharing controls).
That's what personal injury care coordination actually looks like in practice. Not a slogan — a chiropractic referral workflow built around shared context, closed loops, and a referral that
arrives with a reason. A patient who arrives with a history. A specialist who can spend the appointment moving care forward instead of starting over.
What Changes for Each Provider in the Chain
For the referring chiropractor: You send the referral through a digital flow. You include your clinical reason. You can see when the specialist accepts it, when they view the patient's records, when the patient is connected. You're not wondering whether your fax went through. For the orthopedist or pain management provider in the middle: You receive referrals with context attached. You're not starting from scratch. You can access the patient's prior intake findings and records library before the visit. When you refer on to a spine surgeon, you send that context forward. For the spine surgeon at the end of the chain: You receive a new patient who already has organized records on the platform. Their intake is done — often before they walk in. The referring provider's reason is documented. You know why this patient is in front of you. For the patient: They told their story once. It travels with them.How to Reduce Referral Leakage in Personal-Injury Practices
Referral leakage in personal-injury chains isn't inevitable. It's a product of a workflow designed for a world where fax was the only option. That world hasn't been true for a long time — but the workflow hasn't caught up.
Knowing how to reduce referral leakage starts with identifying where handoffs break down: no confirmation loop, no shared records access, no patient-to-specialist connection at the point of referral. A digital referral system for personal injury practices addresses all three — without requiring everyone to be on the same EHR.
It requires a shared layer where referrals carry context, patients are automatically connected to receiving providers, and every party in the chain has visibility into where the handoff stands. That's a solvable problem. PatientPreVue solves it.
The specialist referral workflow in personal-injury cases involves too many handoffs and too much at stake to rely on a fax machine and a hope.
Ready to close the loop on your referrals? See how PatientPreVue's connected-care layer works for personal-injury care chains at patientprevue.com/for-providers.